Dislocation of the patella (patellar luxation)
Patellar dislocation is not an uncommon knee injury, with six events per 100,000 population. The dislocation of the patella often occurs on the basis of a soft tissue or bony pathology (disease/change). After the dislocation, a decision must be made quickly as to whether conservative or surgical therapy is required. The procedure for the first dislocation is still controversial. During the course of treatment, it is important to avoid further dislocations, as otherwise functional limitations and cartilage damage to the knee may result.
In surgical therapy, the pathology must be eliminated in order to ensure the stable running of the patella in the future. There are a variety of options available for this, which must be used in a targeted manner. These include suturing of the MPFL (medial patellofemoral ligament), plastic surgery of the MPFL, axis corrections, reshaping of the gliding groove (trochleoplasty), and modification of the patellar tendon insertion (offset of the tibial tuberosity).
Finding the right procedure
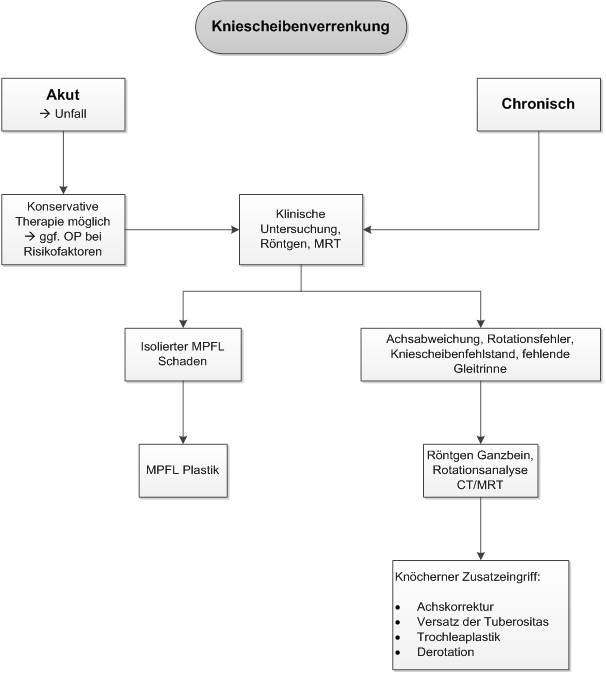
Which procedure - conservative or surgical - is chosen depends on the medical history, the mechanism of the accident, the clinical examination, and the imaging. If there is a first dislocation, and the clinical and radiological examination show no evidence of instability of the patella, an attempt at therapy without surgery can also be made. But here, too, a precise follow-up treatment concept must be followed. As after operations, treatment in the orthosis and a precise physiotherapy concept are also planned here.
MPFL (medial patellofemoral ligament)

In surgical interventions, the so-called MPFL (medial patellofemoral ligament) is the focus of treatment, because it is the main stabiliser of the patella (kneecap) in flexion degrees close to extension and works against a large part of the outward forces. This ligament is torn in about 90% of cases after a patellar dislocation. During the operation, it is replaced by a tendon from the patient's own body (gracilis or quadriceps tendon), which is tensioned in the course of the MPFL. If there are other factors that promote instability, these are also included in the therapy. For example, it may be necessary to create a new sliding groove in the femur for the kneecap in order to achieve bony stability.
